










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares en
SciELO
Similares en
SciELO Compartir

 Permalink
PermalinkRevista Científica Ciencia Médica
versión impresa ISSN 1817-7433versión On-line ISSN 2220-2234
Rev Cient Cienc Méd vol.25 no.1 Cochabamba set. 2022 Epub 31-Sep-2022
https://doi.org/10.51581/rccm.v25i1.466
Articles
MEDICATION, NOCTURNAL DIPPING PROFILE AND HYPERTENSIVE EMERGENCY
1Clinical Intern, King George Hospital, Visakhapatnam, India
2University of Zagreb, Faculty of Medicine, Croatia.
3Merkur Clinical Hospital, Zagreb, Croatia
4University Hospital Center Zagreb Croatia
Introducción:
El objetivo de este estudio fue analizar la medicación utilizada por los pacientes con crisis hipertensiva (presión arterial superior a 180/120mmHg) y su impacto en los principales factores de riesgo para el desarrollo de la emergencia hipertensiva.
Métodos:
Un total de 233 pacientes (108 hombres, 125 mujeres), 184 tenían urgencia hipertensiva/ 53 emergencia (54,44% /50,95% en mujeres) en el servicio de Urgencias durante 11 meses. Los pacientes fueron divididos en cinco grupos de edad según décadas a partir de los 40 años (media de 65,85 años) y un total de diez grupos según el tipo de medicación hipertensiva que utilizaban (IECA ARA, BB, BCC, diuréticos, moxonidina y sus combinaciones).
Resultados:
Utilizando monoterapia antihipertensiva el porcentaje de urgencias hipertensivas fue del 100,00%, 50,00%, 41,66%, 33,33%, 21,05%. El uso de IECA + BCC + diuréticos disminuyó significativamente el número de urgencias al 0%, 18,47%, 21,05%, 25,00%, 33,33%; pero la adición de betabloqueantes disminuyó el riesgo. En general, 53 pacientes no tenían medicación (22,75%) y 68 de 233 pacientes eran fumadores (29,18%, 63,23% hombres), de los cuales 36 pacientes tuvieron una urgencia hipertensiva (52,94% de los fumadores). El mayor número de hipertensos no inmersivos se encontró en los pacientes que tomaban ARA, diuréticos y/o BCC, pero el menor número se mostró en los pacientes que tomaban IECA en combinación con moxonidina (-20,07%). El 22,02% de los fumadores no eran hipertensos inmersivos (-54,67% de los no fumadores). El odds ratio para obtener una emergencia hipertensiva en caso de que el paciente tuviera un perfil no inmersivo fue de 4,18 (IC 1,02 - 18,89, p < 0,05). Los pacientes que tomaban una medicación diferente (o ninguna) no tenían mayor probabilidad de desarrollar una emergencia hipertensiva (OR 1,21, p = NS). No se encontraron diferencias en la incidencia de perfil no inmersivo entre géneros (72,12% varones, 72,83% mujeres).
Conclusión:
Las combinaciones de toda la medicación antihipertensiva mostraron beneficios sobre la monoterapia. Una mayor presión arterial de 24 horas y nocturna (perfil de hipertensión no inmersiva) se asoció significativamente con un mayor cambio para desarrollar una emergencia hipertensiva.
Palabras clave: Emergencia; Hipertensión
Introduction:
The aim of this study was to analyze the medication used by the patients with hypertensive crisis (blood pressure above l80/l20mmHg) and its impact on the main risk factors for hypertensive emergency development.
Methods:
A total of 233 patients (108 male, 125 female), 184 had hypertensive urgency/ 53 emergency (54.44% /50.95% in women) at the Emergency department during 11 months. Patients were divided in five age groups as decades starting from the age of 40 (mean 65.85 years) and a total ten groups depending on which type of hypertensive medication they were using (ACEi, ARB, BB, CCB, diuretics, moxonidine, and their combinations).
Results:
By using antihypertensive monotherapy percentage of hypertensive emergencies were 100.00%, 50.00%, 41.66%, 33.33%, 21.05%. Using ACEi + CCB + diuretic significantly decreased the number of emergencies to 0%, 18.47%, 21.05%, 25.00%, 33.33%; but adding beta blocker additionally diminished the risk. Overall 53 patients had no medication (22.75%) and 68 of 233 patients were smokers (29.18%, 63.23% male) of which 36 patients had hypertensive emergency (52.94% of smokers). The biggest number of non-dippers was found in patients who took ARBs, diuretics and/or CCB but the smallest number was shown in patients who took ACEi in combination with moxonidine (-20.07%). 22.02% of smokers were non-dippers (-54.67% nonsmokers). Odds ratio for getting hypertensive emergency in case patient had a non-dipper profile was 4.18 (CI 1.02 - 18.89, p < 0.05). Patients taking different medication (or none) did not have increased chance for hypertensive emergency development (OR 1.21, p = NS). We didn’t find any differences in the non-dipping profile incidence between genders (72.12% males, 72.83% females).
Conclusion:
Combinations of all antihypertensive medication showed benefit over monotherapy. Higher 24-hour and nighttime blood pressure (non-dipping profile) was significantly associated with greater change for developing hypertensive emergency.
Keywords: Emergency; Hypertension
INTRODUCTION
Guidelines unanimously recommend ambulatory blood pressure (BP) monitoring for BP assessment. However, which BP index among the multitude of measurements that can be derived from conventional and ambulatory BP recordings is more closely associated with adverse health outcomes remains question1.
The nocturnal dipping profile, as a physiological blood pressure (BP) drop of 1020% during the night, is associated with the severity of end-organ injury. Non-dipper profile today is considered to be the cardiovascular risk factor2. The absence of nocturnal BP drop can be caused by abnormalities in extracellular volume or vascular resistance regulation such as increased sympathetic neural tone2,3. Also, sleep disturbances can have an important role in the non-dipper pathogenesis (eg. Sleep apnea syndrome)4. Even mild sleep apnea can increase nocturnal BP by changing the neural tone during the night5. Even though there is no consensus which medication has the greatest impact on restoring the nocturnal BP drop, administering antihypertensive drugs before sleep can improve dipping pattern (eg. Chronotherapy)3,6.
Hypertensive crisis is a common result of uncontrolled hypertension7. It is defined as a systolic blood pressure above 180mmHg or a diastolic blood pressure above 120mmHg8. We differentiate hypertensive urgency without endorgan damage, just as hypertensive emergency in which we have evidence of cardiac, renal, pulmonary or renal injury9. Almost every patient with hypertensive emergency needs to be admitted to the hospital.
The sudden elevation in blood pressure in hypertensive crisis comes from a sudden increase of systemic vascular pressure, due to the action of humoral vasoconstrictors leading to intimal proliferation and fibrinoid necrosis of the blood vessel wall7. According to the last guidelines from ESC (European Society of Cardiology) and ESH (European Society of Hypertension), arterial stiffness is recognized as a risk factor for development of hypertensionmediated organ damage (HMOD) with a pulse wave velocity (PWV) >10 m/s1. PWV is considered one of the most important clinical parameters for evaluation of cardiovascular risk and vascular adaptability and for follow up after the treatment. In previously article we have showed that the measurement of arterial stiffness in an emergency room setting as a noninvasive method of assessing cardiovascular risk in patients with hypertensive urgency10.
The aim of this study was to analyze the medication used by the patients with hypertensive crisis and its impact on the main risk factors for hypertensive crisis development.
MATERIALS AND METHODS
The type of study is observational, descriptive of longitudinal cut, the type of sampling is nonprobabilistic, by convenience. Group of 233 patients (108 male, 125 female) were observed at the Emergency department (ED) in Clinical hospital Merkur with hypertensive crisis from January to November 2019. Past medical history was obtained in ED by direct interview of study participants. Only patients who have been smoking more than 10 years were defined as smokers. Patients were divided into two main groups depending on existing organ damage due to hypertensive episode in ED which lead to hypertensive emergency. In this category we included patients with irreversible damage of the brain (any neurological symptom), kidney (acute kidney failure), aorta (dissection), lungs (pulmonary edema), heart (acute coronary syndrome) or epistaxis. Patients with hypertensive urgency showed no damage on any previously mentioned organ system. Additionally, patients were divided in five age groups as decades starting from the age of 40 (mean 65.85 years) and a total ten groups depending on which type of hypertensive medication they were using: angiotensin converting enzyme (ACE), angiotensin receptor blockers (ARB), beta-blockers (BB), calcium channel blockers (CCB), diuretics, moxonidine; and fixed combination of ACEi + CCB, ACEi + CCB + diuretics with and without BB and moxonidine. Because of too many possible variables, doses of taken medication were not taken into account. All described changes could be dose-dependent but the majority of our patients was put on moderate antihypertensive medication dosages (eg. ACEI-perindopril 5mg, diuretic-indapamide 1.25mg, CCB-amlodipine 5mg, etc.).
BP and pulse wave velocity measurement:
Physicians obtained the conventional readings with a validated auscultator or oscillometric devices (Omron). An appropriate sized cuff was used to the patient's nondominant arm. Patients were considered to have hypertension if their conventional/office BP was 140/90 mm Hg or higher or if they were taking antihypertensive drugs. Inclusion criteria followed the definition of hypertensive crisis as values of systolic blood pressure above urgencies through age groups, males had 72.41%, 47.00%, 44.00%, 41.00%, 11.70%, but more pronounced differences were found in hypertensive emergencies where males had 100.00%, 66.67%, 58.33%, 42.10%, 25.00%. Prevalence of hypertensive crisis in women is obviously rising by aging and is more prominent after the age of 65 compared to men in the same age. Comparing these age group by the medication patients used, preventive drug combination from hypertensive emergency development was found. By using antihypertensive monotherapy percentage of hypertensive emergencies were 100.00%, 50.00%, 41.66%, 33.33%, 21.05%. Using ACEi + CBB + diuretic significantly decreased the number of emergencies to 0%, 18.47%, 21.05%, 25.00%, 33.33%; but adding BB to this drug list additionally diminished the risk of hypertensive development to 0%, 0%, 10.53%, 25.00%, 33.33% in each age group. Overall 53 patients didn't use any prescribed medication (22.75%) and 68 of 233 patients were smokers (29.18%) of which 36 patients had hypertensive emergency (52.94% of smokers). In the smokers group, 43 patients were male (63.23%).
To see the benefit (e.g. Developing less hypertensive emergencies)from taking different medication we created the hypertensive emergency ratio, calculated by dividing the number of hypertensive emergencies with all hypertensive crises in the same category of taking or not taking certain antihypertensive drug (table 1). BB and diuretics showed the highest increase in hypertensive emergency development, while ARBs and moxonidine decreased the ratio by more than 10%. Smokers had 6.26% more emergencies than nonsmokers.
Table 1 Ratio of hypertensive emergency in crisis depending on taken medication
| Medication | Not taking | Taking | Difference | Users |
|---|---|---|---|---|
| ACEi | 22.83% | 21.81% | -1.02% | 110 |
| ARB | 24.48% | 12.19% | -12.29% | 41 |
| BB | 20.63% | 24.32% | +3.69% | 111 |
| CCB | 24.14% | 20.66% | -3.48% | 121 |
| Diuretics | 21.74% | 23.23% | +1.49% | 99 |
| Moxonidine | 25.39% | 10.42% | -14.97% | 48 |
| ACEi + CCB | 25.92% | 17.64% | -8.28% | 102 |
| ACEi + CCB + diuretic | 23.52% | 19.40% | -4.12% | 67 |
| ACEi + CCB + diuretic + BB | 23.16% | 19.15% | -4.01% | 47 |
| ACEi + CCB + diuretic + BB + moxonidine | 23.29% | 11.11% | -12.18% | 18 |
| Smokers | 27.07% | 33.33% | +6.26% | 36 |
Source: author’s own elaboration
Looking on the nocturnal dipping profile, the biggest number of non-dippers was found in patients who took ARBs, diuretics and/or calcium channel blockers. The smallest number of non-dippers were shown in patients who took ACEi in combination with moxonidine (-20.07%). Surprisingly, less than one fourth of smokers were non-dippers (22.02%) which showed the difference of -54.67% compared to the non-smokers. Combinations of all antihypertensive medication showed benefit over monotherapy (table 2). Odds ratio for getting hypertensive emergency in case patient had a non-dipper profile was 4.18 (CI 1.02 - 18.89, p < 0.05). Furthermore, patients taking different medication (or none) did not have increased chance for hypertensive emergency development (OR 1.21, p = NS). We didn't find any differences in the non-dipping profile incidence between genders (72.12% males, 72.83% females).
Table 2 Nocturnal dipping profile depending on taken medication
| Medication | Non dipper (not taking) | Non dipper (taking) | Difference | Users |
|---|---|---|---|---|
| ACEi | 77.14% | 68.05% | -9.09% | 110 |
| ARB | 69.37% | 83.87% | +14.50% | 41 |
| BB | 74.28% | 70.83% | -3.45% | 111 |
| CCB | 69.49% | 74.69% | +5.20% | 121 |
| Diuretics | 66.66% | 79.68% | +13.02% | 99 |
| Moxonidine | 74.28% | 67.57% | -6.71% | 48 |
| ACEi + moxonidine | 76.07% | 56.00% | -20.07% | 28 |
| ACEi + CCB | 73.13% | 72.00% | -1.13% | 102 |
| ACEi + CCB + diuretic | 70.96% | 75.51% | +4.55% | 67 |
| ACEi + CCB + diuretic + BB | 74.07% | 67.64% | -6.43% | 47 |
| ACEi + CCB + diuretic + BB + moxonidine | 74.01% | 60.00% | -14.01% | 18 |
| Smokers | 76.69% | 22.02% | -54.67% | 68 |
Source: authors own elaboration
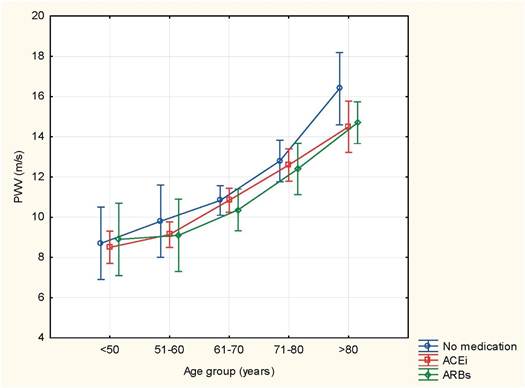
Pulse wave velocity (PWV) was measured in all patients, but the most prominent results were found in patients taking ACEi, ARBs or none. Compared to the same age group ARBs showed the lowest PWV values while patients without medication showed the highest (image 1). Only moxonidine and BB did not show a decrease in PWV values (p=NS, respectively) while adding other antihypertensives reduced PWV values. Smokers had comparable PWV values to nonsmoker patients (p=NS). Average brachial systolic blood pressure was 190.87±9.61 mmHg, Average brachial diastolic pressure was 108.91 ± 16.23 mmHg. Average central systolic blood pressure was 155.34±19.61 mmHg, and average central diastolic blood pressure was 102.86±17.14 mmHg. Values of PWV were higher than reference values for their age in all patients, averaging at 10.71±1.96 m/s. PWV values show positive correlation with age (r=0.9461, p<0.0001)
DISCUSSION
For more than 30 years, ambulatory BP monitoring developed as the most recommended technique for BP measurement (14). ABPM is considered as the preferred approach for measuring BP in guidelines from around the world, but it is still unclear which specific measure is most predictive of adverse outcomes12. Study of Yang WY et all, strengthened the notion that night-time BP measurements carry valuable prognostic information. For every 20/10-mm Hg rise in night-time systolic pressure, total mortality was increased by a relative 23% (HR 1.23; 95% CI 1.17-1.28) and CV events were increased by a relative 36% (HR 1.36; 95% CI 1.30-1.43). Findings were similar when using diastolic readings12. Nocturnal hypertension is of particular interest due to its predictive value in cardiovascular and all-cause mortality outcomes2.
Hypertensive crises seems to be more common in women due to the higher incidence of somatic disorders in them. Despite the slowing heart rate effect, which seems to be an independent risk factor for developing hypertensive emergency, beta blockers increased the number of hypertensive emergencies due to the immune system facilitation. Many immune system cells, especially monocytes in patients with changes on AT1 receptors can increase the oxidative stress in smooth muscles of the vessels15. On the other hand, aforementioned could be the explanation why ARBs reduced the number of episodes. Pathophysiologically, reactive oxidative stress products such as TNFa and IL1 decrease natriuresis by inhibiting NO synthase 3 causing an increase of sodium concentration in blood plasma15. Moxonidine didn't show any impact on the immune system and consequently decreased the number of hypertensive emergencies by lowering the average heart rate (75.71 vs. 82.91 bpm, p = 0.02).
Studies connect nocturnal dipping profile with increased sympathetic nervous system activity during the night16. The most reasonable and common explanation could be the presence of the concomitant obstructive sleep apnea syndrome which alters the activity of sympathetic and parasympathetic nervous system during the night3. Many patients do not present the nocturnal heart rate drop and their diastolic blood pressure is often high during early morning hours. According to these theses, beta blockers and moxonidine showed to be useful in restoring nocturnal dipping profile. Combinations of all anti hypertensive medication showed benefit over monotherapy. Higher 24-hour and nighttime blood pressure (non-dipping profile) was significantly associated with greater chance for developing hypertensive emergency.
Chronotherapy remains an important area of research in hypertension and nighttime administration of antihypertensives improved overall 24-h blood pressure profiles regardless of disease comorbidity6,12. However, inconsistencies between studies suggest a need for more prospective randomized controlled trials with sufficient statistical power.
Our study presented more hypertensive emergency episodes in non-dippers and females but there were no differences between genders in the non-dipping incidence. Nondipping profile combined with somatoform disorders or increased sympathetic neural tone per se seems to be the most dangerous duo for creating end-organ injury. Since a part of the patients included in this study presented with HU as a first manifestation of AH without an earlier diagnosis of AH, measuring PWV allows for the assessment of cardiovascular status for these patients.
The speed at which blood pressure rises is more important than the duration of hypertension for the occurrence of vascular injury1. From the data it was visible that PWV remained elevated despite therapy. However, the method of measuring arterial stiffness is still not the first choice in an ED it takes more time than the classical blood pressure measurement10. Further advancements in technology can lead to improvement in this area.
CONCLUSION
In high risk patients' hypertensive emergencies can be successfully prevented by combined antihypertensive therapy which includes ACEi/ARB, CCB, diuretic and BB, especially in younger age. ARBs and diuretics in monotherapy showed the worse profile in restoring the nocturnal dipping profile. Moxonidine and its combinations with other antihypertensives, especially ACEi, are the most effective medication in restoring nocturnal dip. Dippers had a decreased chance for hypertensive emergency development which pronounce the importance of restoring the nocturnal dipping profile in all hypertensive patients.
In this population-based cohort study, higher 24-hour and nighttime BP were significantly associated with greater risks of HK. Thus, 24-hour and nighttime blood pressure may be considered optimal measurements for estimating cardiovascular risk. Noninvasive measurement of arterial stiffness and nondipping profile in ABPM could be a novel methods in the diagnostic algorithm for patients with hypertensive crisis10.
Limitations
This study has several limitations. First, all patients did not have an ABPM. Among some patients, night-time BP was the time- weighted average of only 3 readings, which is less than proposed by guidelines12. Second, antihypertensive drug treatment was only recorded at baseline and could therefore not be adjusted for as a time-dependent variable.
REFERENCES
1. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al; Grupo de documentos científicos de la ESC. Directrices 2018 de la ESC/ESH para el manejo de la hipertensión arterial. Eur Heart J. 2018 ;39(33):3021-3104. https://doi.org/10.1093/eurheartj/ehy339 [ Links ]
2. Thoonkuzhy C, Rahman M. New Insights on Chronotherapy in Hypertension: ¿El momento lo es todo? Curr Hypertens Rep 2020; 22(4):32. [ Links ]
3. Prkacin I, Balenovic D, Djermovic-Dobrota V, Lukac I, Drazic P, Pranjic IK. Hipertensión resistente y cronoterapia. Mater Sociomed. 2015;27(2):118-21. doi: 10.5455/msm.2015.27.118-121 [ Links ]
4. Birkenhager AM, van den Meiracker AH. Causas y consecuencias de un perfil de presión arterial no descendente. The Netherlands Journal of Medicine. 2007;65(4): 127-131. [ Links ]
5. Wolf J, Hering D, Narkiewicz K. Non-dipping Pattern of Hypertension and Obstructive Sleep Apnea Syndrome. Hypertens Res. 2010, Sep;33(9): 867-71. DOI: 10.1038/hr.2010.153 [ Links ]
6. Bowles NP, Thosar SS, Herzig MX, Shea SA. Cronoterapia para la hipertensión. Curr Hypertens Rep 2018; 20(11):97. doi: 10.1007/s11906-018-0897-4. [ Links ]
7. Rodríguez M, Kumar S, De Caro M. Hypertensive Crisis. Cardiology in Review. 2010;18(2):102-107. DOI: 10.1097/CRD.0b013e3181c307b7, PMID: 20160537 [ Links ]
8. Saguner AM, Dur S, Perrig M, Schiemann U, Stuck AE, Burgi U, et al. Risk Factors Promoting Hypertensive Crises: Evidence From a Longitudinal Study. American Journal of Hypertension. 2010; 23(7):775-780. DOI: 10.1038/ajh.2010.71 [ Links ]
9. Vamsi V, Kamath P, Achappa B, Prkacin I. Redefiniendo la urgencia hipertensiva y la emergencia hipertensiva maligna. Rev Cient Cienc Méd [Internet]. 2019 [citado 2019 Dic 15] ; 22( 1 ): 77-78. Disponible en: http://www.scielo.org.bo/scielo.php?script=sci_arttext& pid=S1817-74332019000100015& lng=es& nrm=iso& tlng=en (10 de julio de 2019). [ Links ]
10. Bilinovac L, Kurjakovic I, Vukovic J, Jug J, Lovric-Bencic M, Prkacin I. Oscillometric Measurement of Pulse Wave Velocity in Hypertensive Crisis. Cardiol Croat. 2020;15(1-2):22-6. | https://doi.org/10.15836/ccar2020.22 [ Links ]
11. Declaración de Helsinki de la Asociación Médica Mundial: principios éticos para la investigación médica en seres humanos. JAMA. 2013;310(20):2191-2194. doi: 10.1001/jama.2013.281053. [ Links ]
12. Yang WY, Thijs L, Zhang ZY, et al. ; International Database; on Ambulatory blood pressure in relation to Cardiovascular Outcomes (IDACO) Investigators. Propuesta basada en la evidencia para el número de lecturas ambulatorias requeridas para evaluar el nivel de presión arterial en entornos de investigación: un análisis de la base de datos IDACO. Blood Press. 2018;27(6):341-350. doi: 10.1080/08037051.2018.1476057 [ Links ]
13. Agedio B900. Disponible en: https://agedio.com/de/produkte/b900.html [ Links ]
14. O'Brien E, Parati G, Stergiou G, et al. ; European Society of Hypertension Working Group on Blood Pressure Monitoring . European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31(9):1731-1768. doi: 10.1097/HJH.0b013e328363e964 [ Links ]
15. Rudemiller NP, Crowley SD. Interacciones entre el sistema inmunitario y el sistema renina-angiotensina en la hipertensión. Hypertension. 2016, Jun;68:289-296. DOI: 10.1161/HYPERTENSIONAHA.116.06591 [ Links ]
16. Mahabala C, Kamath P, Bhaskaran U, Pai ND, Pai AU. Antihypertensive therapy: nocturnal dippers and nondippers. Do we treat them differently? Vasc Health Risk aManag. 2013; 9:125-133. DOI: 10.2147/VHRM.S33515, PMID: 23569382 [ Links ]
Received: January 03, 2021; Accepted: August 30, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
