











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Bolivia's historical medical narrative is marked by its indigenous populations' struggle for the recognition of traditional medicine within a healthcare system dominated by Western medicine (hereby referred to as biomedicine). As a result, indigenous healers face an ongoing challenge in asserting the legitimacy and efficacy of their practices, highlighting inequalities in healthcare access and acknowledgment in Bolivia. This division symbolizes a broader cultural and historical split and has been perpetuated by socio-economic status, geographic accessibility, and ethnic diversity, leading to uneven healthcare access.
The election of Evo Morales in 2006 marked a pivotal moment in addressing these disparities in the healthcare system; his government looked for a reform of the system to decolonize health, applying the reformation plan "Para Vivir Bien" (Johnson, 2010). This concept implies living "with dignity", appreciating cultures, spirituality, and community, giving rise to the "salud intercultural" framework, which aims to bridge traditional and biomedical practices through projects such as Salud Familiar Comunitaria Intercultural (SAFCI), based on the principles of social participation, intersectoral cooperation, interculturality, and the idea that healthcare is in all aspects of family and community life (Johnson, 2010). Currently, SAFCI is present in 319 municipalities (Ministerio de Salud y Deportes, 2024). A list of these municipalities was not found, but it is possible to verify its presence in Samaipata for a post of the Health and Sports Ministry about a vaccine program applied in 2017 (Ministerio de Salud y Deportes, 2017). The discourse between traditional medicine and biomedicine has evolved beyond a simple dichotomy, embracing the complexities of medical pluralism, especially in places like Samaipata, Bolivia, where a mosaic of cultural influences meets. By applying Pierre Bourdieu's theoretical frameworks, this research comes to the following research question: "How does medical pluralism influence people's primary healthcare decisions?".
For this research, the focus will be on four key terms: medical pluralism, traditional medicine (TM from now on), biomedicine (BM from now on), and primary healthcare decisions (PHD from now on). The field of medical pluralism is shaped by diversity in terms of culture, socioeconomic factors, and ideologies of healthcare practitioners that delineate the distribution of healthcare resources and influence individuals' health-seeking behaviors (Khalikova, 2021). In general, this concept of medical pluralism encompasses a broad spectrum of healing practices (Amzat & Razum, 2014), yet, in this research, the focus will be on the two medical traditions of TM and BM, which are the most relevant for the Bolivian context. Firstly, TM is prominently defined by the World Health Organization [WHO] as "the total sum of the knowledge, skills, and practices based on the theories, beliefs, and experiences of indigenous to different cultures" (2023, parr.1). Secondly, BM is generally referred to as scientific Western medicine, as it is the kind of medicine that is associated with experimentation at the laboratory rather than the experience of physicians at the clinic (Gaines, 2008).
In addition, the research was limited to people's primary healthcare decisions (PHD), a concept that was defined in the WHO Declaration of Alma-Ata in 1978 as "the first level of contact of individuals, the family and community with national health" (WHO, 1978, article VI). Following Bourdieu's field theory, PHD would not be a rational choice, but a complex interaction between the habitus, the field, and the different capitals (economic, social, and cultural); habitus is a complex structure that structures behavior through different mechanisms, also it is structured by the field, which is the theoretical place where all actors interact (such as State, companies, people, etc.), and also where the capital is produced, that also shapes the person (Collyer et al., 2015). Either way, capital is not only thought of as the classical material capital, but as three types of capital: the economic capital, which is money, properties, etc., the social capital, represented in the form of recognition, and the cultural capital, which is acquired through life, represented through knowledge (Collyer et al., 2015). In line with this conceptualization of the habitus concept, this research will also look at PHD (habitus) in relation to medical pluralism (field) and the positioning of actors within that field (capital).
Methodological design
This study employed quantitative and qualitative methods to encompass two primary components: community perception and local structures. Quantitative data collection utilized a survey ad hoc administered via Google Forms. To ensure quality, we conducted a pilot survey with a handful of respondents to evaluate the relevance of our questions. Once adjusted, it was administered in teams of two and obtained 61 responses. Qualitative data collection was made through semi-structured interviews with relevant figures from various backgrounds and areas of expertise related to healthcare, concentrated on healthcare practitioners and political stakeholders. For qualitative data analysis, we used an integrated approach of open and closed coding methods. As an initial step, open coding was utilized among a selected number of key interviews to establish a general codebook, which was then applied to the remaining qualitative material using the closed coding method. It is essential to note that due to the limited number of responses, the survey results offer an approximation of the community perception of Samaipata.
Results
Medical Pluralism in Samaipata
To analyze medical pluralism as a social field in Samaipata, it is first important to look closer at how the notion of medical pluralism relates to Bourdieu's concept of social fields. This author conceptualizes social fields when writing about the field of television as "a structured social space [...] in which various actors struggle for the transformation or preservation of the field" (Bourdieu, 1998, pp.40-41). However, when using Bourdieu's field theory, human agency inside a social field is not distributed equally. On the contrary, the interplay between the respective social field and power relations positions the individuals unequally throughout the field. Medical pluralism as a field theory in Bourdieu's framework highlights how diverse medical practices coexist and interact within a social field, and the presence and attitudes of the varying practices impact individuals' healthcare choices, practices, and experiences.
In Samaipata, it was observed that BM and TM operate within the same social field of medical pluralism because of the town's unique characteristics of influx of migration and cultural diversity. This is also visible in the survey statistics, where 45% of survey takers indicated that they have ancestors outside of the Florida province, and 14.6% have ancestors who are from outside of Bolivia. Due to this social and cultural fabric, BM is increasingly used by locals as the health infrastructure expands and costs fall, whereas a large influx of alternatively styled foreigners, largely referred to as "hippies" by the local population, brought with them a large inclination to use natural remedies. Based on this, BM or TM cannot be separated into only one subgroup of the population but have to be seen as belonging to the same social field. Understanding medical pluralism as a social field enables an analysis of how structural forces shape its manifestation in Samaipata. This leads the analysis back to Bourdieu's conceptualization of the social field and a focus on the most powerful actors with the greatest agency to affect change in the social field. As a starting point of this analysis, the focus returns to the Salud Intercultural framework as proposed by Bolivia's government, which is arguably the actor with the biggest potential to affect change in the social field of medical pluralism.
While the Salud Intercultural framework holds significant promise in impacting medical pluralism in Bolivia, its effectiveness in enhancing people's access to healthcare and integrating traditional healthcare practices with biomedical practices is far from meeting its potential. Statistics show that from 2011 to 2022, social security coverage for all of Bolivia increased from 31% to 80% (Instituto Nacional de Estadística [INE], 2024). However, there was not as big an increase in the capacity of the healthcare system. From 1997 to 2007, before Morales became president, the number of health care establishments had increased from 2,000 to 3,100. During his 17 years of presidency, the number of clinics and hospitals only increased from 3,100 to 4,000 (INE, 2024). These results reflect that there was an increase in social security compared to other presidential periods, but the infrastructure did not become stronger or increase at the same rate.
Even if nominal health coverage increases, without enough healthcare establishments to support all new registrations under the Sistema Único de Salud (Single Health System or SUS), many individuals are not able to receive proper care. Additionally, healthcare practitioners do not have the time or sufficient resources to support a higher number of potential patients properly and effectively. This is reflected in the survey as 87% of survey participants had heard of SUS, but 60% said that the public healthcare system has not improved since Morales began his presidency. Furthermore, 65% reported that they don't use biomedical resources, such as hospitals or pharmacies. Because many people in this rural town knew about SUS, it is shown that the roll-out of SUS was quickly done, which aligns with the statistics of a fast increase in individuals covered by SUS nationally. However, the consensus of most survey participants was that not much has changed in the public healthcare system, and there is dissatisfaction towards biomedical services.
Although statistically, more people have increasing social security concerning their healthcare coverage, qualitative research with individuals who are in power within the healthcare structure of Samaipata echoes the lack of infrastructure and resources in the current health system. Through interviews with key stakeholders, insights are gained into the complex dynamics shaping healthcare decision-making in this context. The most powerful interviewee in the field of politics is Dr. Kramer, a direct health advisor to the regional government in Santa Cruz. His perspective underscores the pivotal role of infrastructure and economic resources in delivering quality healthcare:
"Medicine in all parts of the world needs economic resources. A good doctor is not enough. That good doctor needs to have infrastructure to provide care... to give him supplies... We are condemned to failure and unfortunate health policies. In this country, the percentages designated for health are very low." (M. Kramer, personal communication, 2024)
In this quote, Dr. Kramer emphasizes the critical importance of infrastructure and economic resources in healthcare delivery, which resonates with broader discussions around healthcare access and quality. His assertion that "a good doctor is not enough" highlights the systemic deficiencies that undermine the effectiveness of healthcare services in Samaipata. Despite the dedication and expertise of healthcare professionals, without the necessary support and resources, their ability to provide comprehensive care is severely constrained.
Turning to Samaipata itself, an important local stakeholder is Mr. Herrera, the sub-government official of the province of Florida. His account further elucidates the challenges within the healthcare system, highlighting issues related to hiring management and the instability caused by short-term contracts:
"We, for example, have many problems with human resources. An example of one of the problems is that... we have very good professionals who are hired by the municipality and suddenly, they have one-year contracts, and it is an excellent staff... but they change good professionals and bring us others who start from scratch and are terrible." (P. Herrera, personal communication, 2024)
Here, Herrera's observation regarding the turnover of healthcare professionals due to contractual issues sheds light on the instability within the healthcare workforce. The frequent rotation of staff not only disrupts continuity of care but also weakens the development of expertise and institutional knowledge within healthcare facilities.
The quotes from Kramer and Herrera highlight the broader structural challenges that individuals face when navigating the healthcare system. It was found that this lack of stability and resources leads individuals to seek alternative healthcare options or delay seeking medical treatment altogether, exacerbating health disparities within the community. Traditional medical practitioners may also be hesitant to recommend that their patients complement their treatment with biomedical interventions due to the perceived limitations and shortcomings of the biomedical system. Given the scarcity of resources and the challenges faced by biomedical healthcare providers, traditional practitioners view BM as a resource reserved for severe cases rather than an integrated component of holistic healthcare. Consequently, patients can be less inclined to consider biomedical interventions, relying instead on traditional and home healing practices that they perceive as more reliable and aligned with their cultural beliefs and practices. This demonstrates a lack of health infrastructure and resources in one aspect that perpetuates the continuous divide in operations where TM and BM operate in separate spheres.
Turning away from the general discussion of medical pluralism towards the narrower subfield of primary healthcare in Samaipata, it is not the local or regional government but healthcare practitioners themselves who constitute the most powerful actors in the field of primary healthcare. This is related to the observation that the government's attempt at shifting the relationship between BM and TM is mostly a discourse and has less direct effects in Samaipata itself. As a consequence, primary healthcare remains largely unregulated by the government. On one hand, TM was mostly practiced through personal knowledge in the form of picking up herbs, for example, as it became visible through informal conversations and open questions while conducting the survey. Samaipata Municipality's head of the health department, Dr. Nova, explains how TM practitioners remain largely unregulated because they are not certified by the government. On the other hand, BM is more dependent on the government in theory. However, the lack of infrastructure results in people not consulting doctors before seeking medication. As medical prescriptions are uncommon, people go directly to pharmacists, where they can get anything from small painkillers to strong antibiotics. This process was observed multiple times when conducting interviews at pharmacies. The encounters witnessed between patients and practitioners were short. The patients mentioned their physical condition, and the pharmacist gave them the medication she or he thought best fit the symptoms without any prescription or further check-up.
Ultimately, it is this arrangement of infrastructure in the social field of medical pluralism that puts the pharmacists and traditional medical practitioners in a powerful position. It is the direct views of these healthcare practitioners on the relationship between BM and TM that have particular power in the relationship between the two subfields of medical pluralism.
The influence of healthcare practitioners on primary healthcare decisions
As has been previously discussed, how the social fields impact PHD, the focus now turns to how habitus influences PHD by analyzing the survey results of the general public. From the survey data, it can be seen that biomedical and traditional practitioners do not influence PHD in the same way. Graph 1 compares the PHD (different bar colors) with the type of medical practitioner that people regularly go to (the right graph for traditional practitioners and the left for biomedical practitioners). The x-axis presents people who regularly go or don't go to the corresponding type of practitioner. The y-axis shows the percentage of survey respondents making the corresponding healthcare decisions.
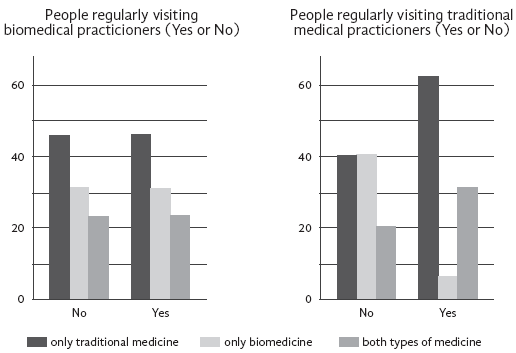
The results of these graphs show the different levels of influence amongst the types of healthcare practitioners. When looking at the left part of Graph 1, one can see that assisting regularly with a biomedical practitioner is practically unrelated to PHD as both groups of people have the same patterns in PHD. However, turning to the right side, it can be seen that people who regularly go to traditional practitioners make different PHD than those who do not regularly go. Overall, this impact is particularly visible for the PHD of "only using traditional healthcare" (60% instead of 40%) and "only using biomedicine" (6% instead of 40%). Turning away from descriptive statistics, the noticed effects of traditional practitioners can also be seen when conducting a linear regression against the PHD of "only using TM", as seen in Table 1. In contrast to the weak association between healthcare decisions and biomedical practitioners (B= 0.06; p= 0.74), traditional practitioners have a clearly stronger association (B= 0.3; p=0.07). This overall means that people going to traditional practitioners are 30% more likely to only use TM for primary healthcare. Indeed, this association is relatively stable with respect to most control variables; only against the control variables education, religion, and age does the p-value rise to around 0.1.
Table 1 Regression analysis predicting PHD based on visits of healthcare practitioners.
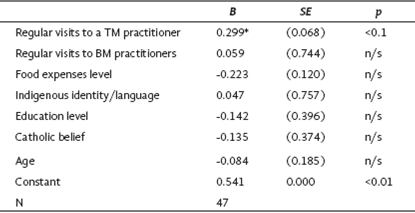
Note: * p<0.1, ** p<0.05, *** p<0.01
These results make it possible to theorize that, unlike the biomedical practitioners, the traditional practitioners are able to impact healthcare decisions to a larger extent. Returning to the qualitative results, this non-influence of biomedical practitioners can be explained through the diversity of opinions amongst pharmacists regarding what constitutes the best combination of primary health care. A pharmacist was encountered who had a more skeptical view towards using TM for primary healthcare: "... I'm not such a believer in traditional medicine..." (Angelica, personal communication, 2024). However, other biomedical professionals were more open to including TM for primary healthcare. One example is Marvin, a pharmacist with his own establishment in the heart of Samaipata, who shared his view on how to integrate traditional remedies with biomedical ones:
"... What do I prescribe to my patients for medication for stomach pain? If that is the case... a prescription comes to the doctor with an antibiotic for it, which is perfect, but apart from that, for example, I recommend that it be an infusion, that is, a little coca or mint tea, and this makes the patient improve..." (Marvin, personal communication, 2024).
Marvin's practice of integrating herbal tea, natural and herbal remedies with conventional antibiotics and other conventional BM emphasizes the potential for an integrated blending of healthcare practices. This means that at least in some biomedical circles in Samaipata, TM and BM are not viewed as isolated medical paradigms but rather as mutually supportive. However, as this opinion is not shared amongst all BM practitioners, it is yet to be decided which group of BM practitioners will gain more dominance in the future.
Contrarily, the perspective from the TM side has a more homogenous opinion on what constitutes the best form of primary healthcare, which can explain the found correlation between the regular visit of traditional practitioners and PHD. A prominent figure amongst these TM practitioners is Juan Carlos, who is the owner of EcoTao, a well-known local center for traditional medicine. He has an overall skeptical position towards BM: "... For the large pharmaceutical industry, the business is in the sick. So, for the big pharmaceutical industry, the business is to keep people sick as long as possible..." (Juan Carlos, personal communication, 2024). This skepticism towards the use of biomedical medication for primary health is directly shared by most of the traditional practitioners encountered in Samaipata. However, Juan Carlos also shared that BM cannot be disregarded because there are "... situations in which one has an accident, there you cannot say we are going to give him herbal tea. There, he requires a surgery..." (Juan Carlos, personal communication, 2024). This point of view indicates a clear boundary for BM's role, which is perceived only as essential in severe health crises, reflecting a more targeted approach rather than an integrated approach to health.
To summarize, the data show that well-positioned powerful actors in the respective social field (in this example, healthcare practitioners) can assert some type of influence on the habitus formation. However, it is seen that the level of homogeneity among the practitioners matters for asserting influence on the population. On one hand, there was no relation between regular visits to biomedical practitioners and PHD, which coincides with the fact that pharmacists in Samaipata have different opinions on what constitutes the ideal type of primary healthcare. On the other hand, there are some statistical relations visible between the regular visit of traditional practitioners and PHD, which connects to the observation that traditional practitioners have a more united opinion when asserting the primacy of herbal medicine.
However, care should be taken not to over exaggerate the extent of power that medical practitioners have on PHD in Samaipata. The data shows people's personal, or family, knowledge is the most used form of healthcare, with 52% of the respondents saying that they regularly use home medicine, in contrast to regular visitors of biomedical (30%) and TM (34%) practitioners. Thus, even though traditional healthcare practitioners hold special influence over their patients, it is important to remember that their patients are a minority of total survey respondents.
The influence of various types of capital
Besides analyzing the influence of medical pluralism with a focus on the most powerful actors of the social field, another important concept in Bourdieu's "field theory" is capital. In order to utilize Bourdieu's notion of capital, it is important to include cultural dimensions in the analysis. Due to the limited scope of this study, the study was narrowed to focus on Bourdieu's various types of capital, specifically economic and cultural capital, and to operationalize it through a few key variables. These variables were selected from the broad list of demographic questions from the survey based on their association with PHD. Firstly, Bourdieu's notion of economic capital refers to distributions in "mercantile exchange," which could be translated as the level of wealth. Therefore, the most relevant was found in the proxy variable level of food expenses. Secondly, the notion of cultural capital, Bourdieu references "the capacity of certain gifted individuals [...] to recognize and appreciate" certain qualities such as well-known references, rules of the game, and the ability to gain the approval of others (Moore, 2012, pp.100-102). Thus, to operationalize cultural capital, the analysis can return to the Medical Pluralism section, where it was seen that the large historical divide in the social field of medical pluralism roots back to the divide between Western and previously present indigenous cultures. This divide is also historically connected to the unequal spread of knowledge, in which indigenous cultures are associated with a greater knowledge of TM. It could be expected that the relevance of cultural capital may express itself through the association between individuals and a particular culture.
To understand the effects of cultural and economic capital on PHD, one can look at Graph 2, which shows that different levels of economic capital create bigger differences in PHD than differences in cultural capital. For example, almost the same percentage of people earn a PHD by only using traditional medicine, independently of either: 1) Their association to indigenous culture (59% percent); or 2) lack of association to indigenous culture (53% percent). On the other hand, 67% percent of people with a low level of wealth make the PHD by only using traditional medicine, compared to 43% percent with a high wealth level. Moving beyond simple descriptive statistics and focusing on linear regressions, economic capital also represents the dominant logic of capital arrangement in the field of medical pluralism, as shown by the following regression table.
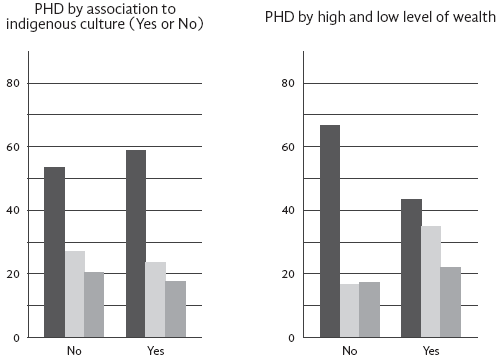
Table 2 Regression analysis predicting PHD Based on the type of capital.
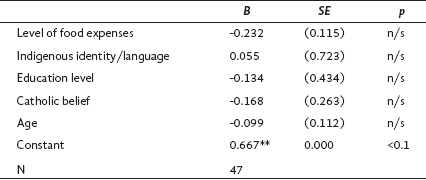
Note: * p<0.1, ** p<0.05, *** p<0.01
The first two regressions in the table above show the relationship between the respective type of capital and PHD without control variables. Here, it can already be seen that PHD has a stronger association with food expenses than with indigenous culture. Food expenses have a stronger correlation coefficient (-0.232 instead of 0.055) and higher statistical significance (p-value of 0.12 instead of 0.72). Turning to the control variables (Education level, Catholic belief, and Age), it can be seen that the strong association between PHD and economic capital is relatively stable with respect to all control variables, education being the strongest influence out of the three control variables (B=-0.134), and age the weakest (B=-0.099).
Following the results of the data analysis, one of the more surprising findings has been that there is no statistically significant correlation between indigenous culture and PHD amongst the residents of Samaipata; instead, economic capital creates the most significant distinction for PHD. Qualitative observations do agree on this affirmation. Samaipata is far from being a traditional indigenous society, a strictly ethnically segregated society, or even simply a rural town; it is instead a modern style developing capitalist society, directly exposed to international flows of people, ideas, and goods, with a tourist-oriented "chic" downtown, and diverse foreign communities from various countries. This is in comparison to nearby agricultural towns such as Mairana, where tourism and foreigners play a less central role; interviewees also confirmed this observation. For example, the Medical Director of the Florida Province stressed how unique Samaipata is, as it is the only town in the province that has tourism as the main driver of its local economy (Romero, personal communication, 2024). In conclusion, it is this integration of the various cultural groups of Samaipata that can explain why the driving logic creating the distinction of habit in the field of medical pluralism is now economic and not cultural capital. Despite this observed trend, it would be incorrect to say that cultural capital does not matter any longer in Samaipata at all. For example, it was observed qualitatively that it was common knowledge that European foreign residents of Samaipata possess a much higher level of economic capital. However, due to the small sample size of people speaking a European language besides Spanish (10), it was not possible to test these qualitative observations quantitatively.
Conclusions
First, the analysis of medical pluralism's manifestation in Samaipata suggests that influential actors within this social field, exemplified here by healthcare practitioners, wield a discernible influence on PHD (i.e., habitus formation). The degree of consensus among practitioners emerges as a pivotal determinant, whereas the frequency of visits to biomedical practitioners fails to correlate with primary healthcare choices. This is related to the inherent diversity of perspectives among pharmacists in Samaipata, so a statistically significant relationship is seen between regular consultations with traditional healers and primary healthcare decision-making. This aligns with the unified position held by TM practitioners in advocating for herbal remedies.
Second, medical pluralism relates to the lack of health infrastructure and resources, which affects the ongoing divide between TM and BM operations. The data analysis reveals that this ongoing divide statistically manifests itself primarily in the form of economic capital, as opposed to cultural capital. A lack of statistically significant correlation between PHD and cultural or linguistic association with indigenous culture was observed among Samaipata residents. Instead, economic capital emerges as the predominant determinant shaping PHD.
This research opens avenues for further inquiry. Future qualitative studies could delve deeper into specific factors driving individuals' relationships to TM and BM, as well as the efficacy of different healthcare interventions within Samaipata. Future quantitative studies could approach the intersection of TM and BM utilization by individuals, providing insights into the evolving dynamics of medical pluralism in healthcare decision-making processes. Additionally, comparative studies across different regions could elucidate variations in healthcare utilization patterns and the underlying determinants of this. Exploring the role of social networks and interpersonal relationships in shaping healthcare decisions could provide a more comprehensive understanding of the complexities inherent in medical pluralism.
Regardless of the research's limitations and the suggestions for further inquiry, an attempt can be made to assert practical implications for healthcare policy and service provision in Samaipata based on the findings. Despite statistical data indicating widespread social security coverage, significant deficiencies in healthcare infrastructure and resources can be observed. This calls for targeted interventions to address these gaps, particularly in rural and marginalized communities. Additionally, the pervasive distrust of TM practitioners highlights the need for efforts to improve the quality of care and rebuild trust among residents. Understanding the influence of economic capital on healthcare decisions emphasizes the importance of ensuring equitable access to healthcare services.

